











































Public Sector Response to Gender-Based Violence in Vietnam
"The training supported through the project had a profound impact on many providers and government partners because it provided opportunities to think critically, for the first time, about gender equality, gender norms, and GBV. Programs should ensure that such training, along with information and guidance for providers, communities, and those experiencing violence, is supported in future projects."
From the Case Study series, AIDS Support and Technical Assistance Resources (AIDSTAR-One) Project, Sector 1, Task Order 1, this report documents Vietnam's Improving Health Care Response to Gender-based Violence project, a public sector intervention that builds on a medical model and links survivors to ongoing counseling and support. As noted here, gender-based violence (GBV) is widely recognised as both a cause and a consequence of HIV infection. However, GBV is underreported and underresearched in Vietnam. "Cultural norms (some might argue based on Confucian philosophy) position Vietnamese women as subservient to their father, husband, or eldest son (after the husband's death)..Vietnam's policies have evolved to reflect the rapidly changing social and economic situation in Vietnam, especially after 1986....However, the laws in and of themselves are not sufficient to begin the process of change....While several decrees and strategy documents have been issued, many are not backed by line item budgets, staff training, or mechanisms to ensure the accountability of those responsible for implementation..."
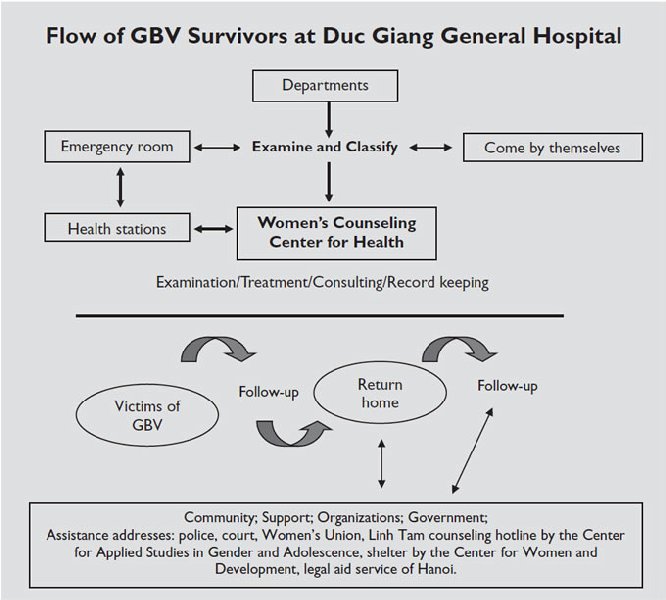
In 2002, with technical assistance from the Center for Studies and Applied Sciences in Gender, Family, Women and Adolescents and the Population Council, and financial support from the Ford Foundation, Hanoi Department of Health Services (HDH) piloted the Improving Health Care Response to Gender-based Violence project. The project model had three components: screening, referrals, and community outreach and support. Phase I took place at Duc Giang General Hospital (DGGH); phase II took place at Dong Anh General Hospital (DAGH). Activities involved:
- Integrating GBV screening into health services: All medical and nursing staff in emergency rooms, obstetrics/gynaecology and surgery departments, maternal and child health and family planning, mobile teams, and other professional staff and managers were trained in basic knowledge about GBV, consequences of violence, recognising GBV, talking to clients, working with survivors, and collaborating with the community to support GBV survivors. Staff were trained to use a short, three-question screening tool asking clients whether they have experienced physical, emotional, or sexual violence, or rape. The training also discussed the issues that underlie GBV in Vietnam, including gender, the unequal power between men and women, the pressure of gender roles, and the causes of GBV.
- Free counselling services: Both hospitals receive GBV referrals from other hospitals, mass organisations, and the police, and accept walk-in clients from the community who hear about the service through mass media or friends. DGGH keeps detailed case reports on each survivor and takes photos of a woman's injuries in case she decides to press charges. The counsellors provide one-on-one counselling and refer women to other services, including reproductive health, a counselling hotline, shelter in Hanoi, and/or community-based organisations that provide support. In phase II of the project, counsellors started advising women who experienced sexual violence and those whose partners refused to use a condom to visit the Voluntary Counseling and Testing Center for HIV testing and counseling (HTC). The HIV and sexually transmitted infection (STI) services are easy to access and free; however, "counselors said that many women were reluctant to test for HIV; only 282 women accepted referrals to the voluntary counseling and testing site at DGGH and only 15 at DAGH (fewer than 10% at each facility).
- Community outreach and support: The Population Council trained hospital and counselling centre staff as master trainers. These trainers visited communities monthly to provide communication sessions on GBV and gender equality to members of mass organisations, like the Farmers' Union and Students' Union, or interested community members. In phase II, "Clubs for Family Happiness" were established for female survivors in several communes, and members of the Women's Union were invited to participate in helping to decrease stigma. In some communes, community members established two different clubs: one for survivors of violence, and one for GBV prevention volunteers. Both clubs provided information on GBV and referrals to counselling centres and trusted addresses. The survivors' club introduced dancing, drama, games, painting, and puppets to help women express their emotions and discuss solutions. Gradually, management of the clubs shifted from project staff to club members, who continued to organise performances in their communities. These clubs aim to provide a safe environment for women to share their problems, support each other, learn how to solve family conflicts, and make safety plans.
"A 2005 assessment by the Population Council and HDH indicated significant positive changes in providers' awareness and attitudes regarding gender equality and factors contributing to violence during phase I (Mai 2006). Findings also indicated more proactive screening, assessment, and documentation of GBV cases, and improved support to GBV survivors. The training strengthened providers' counseling skills and improved their ability to interact with GBV survivors."
What worked well: expanding providers' awareness of GBV; increasing community awareness of GBV; providing training expertise; and presenting a model for a domestic violence law.
Challenges include: limited response to GBV across sectors; limited impact on HIV prevention; economic constraints; staffing; and future funding.
Recommendations include: link HIV and GBV in service provision; establish a broad advocacy base; include males in efforts to reduce GBV (in order to begin changing norms that perpetuate gender inequality and GBV); integrate GBV screening across services; incorporate quality assurance; and foster donor-government collaboration.
Click here to access AIDSTAR-One's Facebook page.
Emails from Anna Lisi to The Communication Initiative on March 6 2012 and March 8 2012; and AIDSTAR-One website, March 7 2012.
- Log in to post comments