











































Understanding the Complexity of Demand-Side Determinants on Vaccine Uptake in Sub-Saharan Africa
Radboud University Medical Centre (van Heemskerken, Broekhuizen); Access-To-Medicines Research Center (Decouttere, Vandaele); Wageningen University and Research (Broekhuizen)
"With vaccination coverage stagnating across SSA, it is critical that the complexity in policy development is confronted."
The complexity of socio-cultural factors impacting vaccine uptake in sub-Saharan Africa (SSA) is not well understood. One of the reasons for low vaccine coverage in SSA is vaccine hesitancy, which varies across time, place, and type of vaccine. This paper reviews the socio-cultural determinants of vaccine uptake and visualises their interrelationships by adopting a systems perspective, where the goal is to understand the complexities that underlie complex adaptive systems by focusing on relationships and circular causality instead of on individual causes and linear causality.
The researchers conducted a literature search of articles published from 2000 to 2019 describing socio-cultural demand-side determinants for vaccine uptake in SSA. Ninety articles, primarily from Nigeria (n = 23), Ethiopia (n = 17) and Kenya (n = 11), met the inclusion criteria.
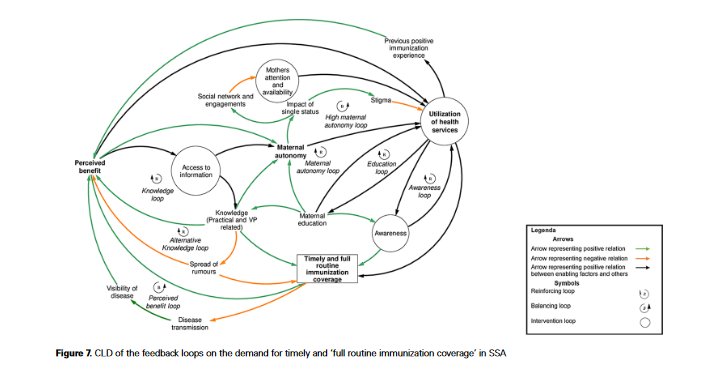
Using the Andersen and Newman Framework of Health Services Utilization, demand-side determinants were categorised as predisposing characteristics (i.e., demographic factors, social structure factors, and health belief factors), enabling resources (personal and community), or need factors (e.g., perceived by the individual based on personal experience). A qualitative system dynamics approach was employed to visualise how these factors and their dynamic interrelationships influence vaccine uptake. This visualisation, by means of a causal-loop diagram (CLD), was mostly based on a qualitative input gleaned from the papers included in the review. Quantification was done by counting direct (statistical) associations between each determinant and 'timely and full routine immunisation coverage'.
From the literature, the researchers identified 25 predisposing factors, 14 enabling resources, and 3 need factors, but they included 23 predisposing factors, 5 enabling resources, and 2 need factors in the CLDs, since supply-related factors were not within this paper's scope. Here are two examples:
- Maternal age (a predisposing factor) impacts demand for vaccination in SSA. For example, a higher maternal age has been found in some research to relate to more experiences with unimmunised children dying of vaccine-preventable diseases and a subsequent better understanding of the importance of vaccinations. This factor can influence feedback loops that are related to perceived benefit. A higher maternal age is also positively associated with access to information about routine vaccination and therefore has a positive impact on knowledge loops.
- Many factors influence and are influenced by maternal autonomy (an enabling resource), such as maternal education, which in turn is increased through maternal practical knowledge about the location of vaccination and knowledge about the vaccination schedule. However, high maternal autonomy is not solely an advantage, which is captured in one of the loops (e.g., depending on the cultural context, the impact of women living alone or being single might result in women feeling stigmatised if they utilise health services).
Most feedback loops involve utilisation of health services with 77 loops, perceived benefit with 73 loops, and maternal autonomy with 66 loops. These large numbers of feedback loops are the result of several alternative pathways through which socio-cultural factors exert their influence on vaccine uptake. For instance, the alternative knowledge loop shows that an increase of knowledge also leads to a decrease in the spread of rumours (e.g., worries about vaccination safety or anti-vaccination messages and plots). The decrease in the spread of rumours increases perceived benefit.
Foci of policy interventions as found in the papers are represented by red circles in Figures 6 and 7 in the paper. Interventions affect different areas of the system. Most demand-related interventions identified in the literature influence access to information, mothers' availability and attention, and/or awareness. For instance, one way to enhance access to information is by using communication channels that were also used for mass vaccination programmes. An example of an intervention that aims at increasing awareness and mothers' availability and attention is providing mothers with calendars.
In short, this analysis revealed that maternal autonomy and the perceived benefits caregivers attach to vaccination exert their influences on many other factors through several feedback loops, thereby influencing timely and full routine immunisation coverage in SSA. More research is needed on autonomy and perceived benefit, which presently have an unclear evidence base but play a central role. Utilisation of health services (supply-related) and access to information (demand-related) are considered high-potential leverage points.
The researchers discuss some issues surrounding the capturing of system maps. For example, gaps in the evidence base can lead to incomplete CLDs. This query did not capture any articles on trust, whereas some papers mentioned it as a critical component in vaccine uptake, and evidence on perceived benefit and maternal autonomy was insufficient. Nevertheless, the latter two seem to play a key role within the CLDs. In addition, many of the identified determinants are maternal-related; evidence on paternal influences or shared decision-making is scarce and requires more research.
There are also some conceptual issues that may make it hard to base a decision on a CLD, such as: indetermination (a policy has both positive and negative influences on the goal), indistinction (multiple policies have same influence on goal), and multiplicity (there are multiple goals). Methods for dealing with these issues are: undertaking topological analysis, assigning strengths to each link, or deliberatively evaluating the CLD and having policymakers vote on each of the policy options.
Next, the researchers explore the possibility of quantitative system models for health technology assessment (HTA), providing a few examples of existing approaches. They suggest that, "[i]f quantification is possible, modellers can use the systems approach to obtain more realistic incremental cost-effectiveness ratios and other expected effects. It can also help to identify leverage points, i.e. components of a system where small changes can have a substantial impact....Even if full quantification is not possible, constructing a systems map can still be valuable as it helps to structure the problem, to serve as a communication device and to identify the limits of quantitative models."
In conclusion: "Straightforward tools such as the one illustrated here are available to increase the usefulness of a systems approach throughout the various stages of policy making, from hypothesis generation to intervention development and evaluation. The results presented in this study can be a stepping stone in this journey. However, significant effort is needed to transform literature-sourced CLDs into country-specific ones and should at least require the involvement of local citizens and experts."
Health Policy and Planning, Volume 37, Issue 2, February 2022, Pages 281-91, https://doi.org/10.1093/heapol/czab139.
- Log in to post comments