











































Effectiveness of a Census-Based Management Information System for Guiding Polio Eradication and Routine Immunization Activities: Evidence from the CORE Group Polio Project in Uttar Pradesh, India
CGPP/India (Choudhary, Solomon); Johns Hopkins Bloomberg School of Public Health (Perry)
"[T]he CGPP CB-MIS has been instrumental for polio eradication and RI activities in high-risk areas of Uttar Pradesh where hard-to-reach and resistant groups are located."
Census-based management information systems (CB-MISs) provide current information about everyone in the population covered by a public health programme. This article assesses the effectiveness of the CORE Group Polio Project (CGPP)/India CB-MIS in the management of social and behaviour change communication (SBCC) interventions, which were ultimately designed to improve polio and routine immunisation (RI) coverage in underserved populations. The article also assesses the feasibility of the CB-MIS for vital events registration and explores the potential of this CB-MIS for contributing to the effectiveness of other public health programmes in similar environments.
The article opens by describing the SBCC work of the United States Agency for International Development (USAID)-funded CGPP (see the other articles in the series of articles on CGPP's contributions to the Global Polio Eradication Initiative (GPEI), accessible through Related Summaries, below). At the centre of CGPP/India's activities is the Social Mobilization Network (SMNet), formed in 2003 to identify high-risk areas and work with underserved communities in planning, implementing, and monitoring social mobiliation and other immunisation-related activities. The activities of the SMNet are carried out by community mobilisation coordinators (CMCs), who are supervised by block mobilisation coordinators (BMCs), who are in turn supervised by district mobilisation coordinators. A network of 1,100 CMCs conducts social mobilisation activities for social and behaviour change related to polio vaccination and RI. When resistance is encountered, the CGPP facilitates engagement with informal and formal community leaders.
The CGPP/India has its own CB-MIS, which contains information on all households and the individuals living in each household in the CGPP catchment areas. This CB-MIS tracks inputs, outputs, processes, and outcomes of its SBCC interventions. Each CMC is responsible for 500 or so households and maintains registers about each of them, including the current vaccination status of every child. In addition to routinely collecting data, the CGPP conducts specific investigations using both quantitative and qualitative techniques, such as lot quality assurance sampling (LQAS) surveys and barrier analysis (to identify barriers families face in adopting healthy behaviours). The CGPP's CB-MIS has evolved over time - from one with only several indicators to a full-fledged system with many indicators built into a log frame. The CGPP log frame provides a summary of interventions, expected results, and a monitoring and evaluation plan for each of the project's objectives. (Figure 1 in the article describes the various registries, tools, and records that make up the CB-MIS; the various levels and stages of data collection, compilation, analysis, and reporting at each operational level; and the flow of information between levels of operation. The Assessment and Evaluation section (at the bottom of Figure 1) lists the various data sources that the CGPP uses for managing the system.)
The article measures the outcomes of the CGPP by observing the trends of vaccination coverage in CGPP catchment areas over time. It uses data from October 2014 to September 2017 that were originally collected for the CB-MIS, including denominator populations, immunisation status of children, and registration of pregnant women, newborns (births), and infant deaths. It also uses 11 years of supplementary immunisation activity (SIA) coverage data (from 2007 to 2017) for areas adjacent to CGPP catchment areas that were compiled through the CB-MIS of the CGPP.
The article also computes vital statistics from births and deaths registered through the CGPP CB-MIS and compares them with the estimates from the Civil Registration System of India, using statistics from India's Sample Registration System in Uttar Pradesh as the "gold standard". The authors estimate that the CGPP's CB-MIS has registered 86% of births and 98% of infant deaths, a much higher level of registration than has been achieved by the Civil Registration System for the entire state of Uttar Pradesh.
In short, the data shared in the article reveal that, "[f]ollowing the introduction of the CB-MIS in the CGPP catchment areas composed of hard-to-reach and resistant populations, there has been an increase in polio campaign coverage, a reduction in the percentage of households that resist polio immunization, and a sustained high level of RI coverage for polio and other antigens." Based on the authors' experience, the following strengths of the CB-MIS have contributed to these achievements:
- "The CB-MIS makes it possible for the CMCs to create micro-plans based on solid household-level information at the community level.
- Complete information is available for each child identified by household, enabling CMCs to implement CGPP interventions better.
- The dual recordkeeping system of information compiled at CMC and BMC levels enables the use of information for both interventions at the household/community level (using disaggregated data) and management at the block level and higher (using aggregated data). Duplicate carbon copies of the monthly performance reports, which provide basic data such as number of live births and number of children vaccinated, are shared by CMCs/BMCs with their immediate supervisors. These data are not only used for reporting but are also used by the supervisors for validation.
- The information is collected, compiled, and analyzed by the frontline workers (CMCs and BMCs) with minimum technical support, empowering them to improve the effectiveness of their own work.
- The standardized templates for data compilation and analysis facilitate timely feedback to frontline workers and enable them to use this information for planning and implementation at their level."
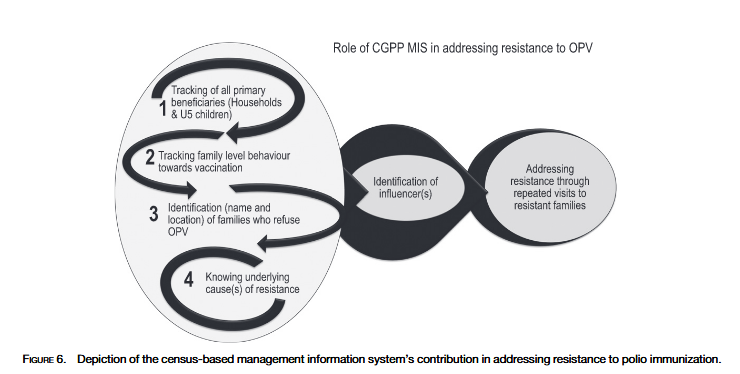
As detailed here, the CB-MIS has enabled community-based health workers to make behavioural diagnoses of barriers to immunisation and to overcome them; this capacity is not possible for an MIS that relies on sampled households. For example, armed with information, CMCs are able to investigate the reason(s) behind oral polio vaccine (OPV) refusal by having personal interactions during home visits to each resistant family. The potentially resistant households may include families with a history of an adverse event following immunisation (AEFI), families belonging to an area where a severe adverse event was reported, or families from an area where an anti-vaccination group has actively disseminated messages in the form of fatwa. Having identified resistant or potentially resistant families and appropriate influencers, CGPP field staff (mainly CMCs and BMCs) and influencers visit the families repeatedly, if necessary.
In conclusion: "The CB-MIS, originally designed for CGPP India, has been replicated in other CGPP countries. For instance, the CGPP in Nigeria has adopted the child tracking system to effectively execute polio campaigns and RI services. It could be adopted for other public health programs where case detection and follow-up are necessary, such as child survival programs or tuberculosis programs."
American Journal of Tropical Medicine and Hygiene, 101(Suppl 4), 2019, pp. 33-44. https://doi.org/10.4269/ajtmh.18-0935
- Log in to post comments